The Cost of HIV Medications in the Illinois Health Insurance Marketplace
|
|
|
- Nigel Stewart
- 6 years ago
- Views:
Transcription
1 The Cost of HIV Medications in the Illinois Health Insurance Marketplace June 15, 2015 To help people with HIV choose health insurance marketplace plans, the AIDS Foundation of Chicago (AFC) has collected information on HIV medication coverage for each plan. This document gives examples of what a person with HIV might pay for HIV medications. Keep in mind: Do not rely solely on the information in this document to choose a plan it is only a guide. Consult a trained enrollment assister for help in selecting a plan. You can reach an AFC Medical Benefits Coordinator at Always verify medication coverage directly with a plan before enrolling. Insurance companies can change their coverage without telling consumers. We only looked at the cost and coverage of a few HIV medications. Contact the plans directly if you take medications that are not listed here. Open Enrollment ended on Sunday, Feb. 15, A Special Enrollment Period (SEP) may apply if you have had a significant change in circumstances. Please contact an AFC Medical Benefits Coordinator at to discuss whether you may qualify for a SEP. The Illinois Medication Assistance Program (MAP) (formerly ADAP) and the Premium Assistance Program (PAP-formerly CHIC) can help! If you sign up for the MAP and/or PAP and enroll in a coordinating plan, you won t pay premiums or any out-of-pocket costs for HIV medications. Read more about MAP below. Please be reminded that MAP pays for the medication portions, PAP pays for the premiums. Need help choosing a plan? For help applying for coverage, either Marketplace plans or Medicaid, please contact an AFC Medical Benefits Coordinator at All coordinators are familiar with the unique concerns of people impacted by HIV. HIV medications are in many cases unaffordable AFC s analysis shows that four companies Assurant, BlueCross BlueShield, Land of Lincoln, and offer HIV medications with affordable out-of-pocket costs. In many of these four companies plans, a complete HIV regimen would cost $35-$150 per month. However, HIV medications are far more expensive and likely unaffordable for nearly all people with HIV in Coventry, and, Humana plans. In many cases, HIV medications are on the highest medication tier, requiring a coinsurance payment of as much as 50%. Coventry has moved HIV medications to more affordable tiers effective June 1, This document has been updated to reflect those changes.
2 Concerted advocacy will be needed to ensure that HIV medications are affordable in all plans. AFC is committed to leading this advocacy at the state and federal levels. The Illinois Medication Assistance Program (MAP) can help! Fortunately, the Illinois Medication Assistance Program (MAP-formerly ADAP) and the Premium Assistance Program (PAP-formerly CHIC) can help people with HIV afford medications on plans purchased through the marketplace. The Medication Assistance Program covers these costs because successfully treating HIV has significant benefits for individuals with HIV, as well as the community. People with HIV who have an undetectable viral load have better health outcomes. Moreover, they are far less likely to transmit HIV in the community. People enrolled in the Medication and Premium Assistance Programs won t pay monthly premiums or any out-of-pocket costs for HIV medications that are part of the MAP Program Formulary which currently contains 158 medications. However, to benefit from these programs, you must select a Silver, Gold or Platinum plan from one of these insurance companies: Assurant Health BlueCross BlueShield In addition, the Premium Assistance Program requires that the annual premium cost plus the maximum out-of-pocket cost for the selected plan cannot exceed $10,482 per client per year. If you are eligible for the Medication and Premium Assistance Program you must select one of these plans in order to receive any benefits. To apply or for more information about the programs, including eligibility requirements, contact MAP/PAP at or visit iladap.providecm.net. Pre-Exposure Prophylaxis (PrEP) People who are not infected with HIV may be able to take a medication to help prevent infection. Currently only one medication, Truvada, is approved for this use. The monthly cost of Truvada can be found in this document It can also be found using the plan information below and is the same cost as Truvada used to treat HIV. To date, AFC has not heard reports of insurance companies denying coverage of Truvada as PrEP. For more information on insurance company coverage of Truvada for PrEP, visit Important notes The regimens we chose to examine are the recommended regimens according to the Department of Health and Human Services. (Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Department of Health and Human Services.) We have also included all available single tablet regimens.
3 All coverage information was accessed between November 10 and December 1, 2014 and updated on June 15, 2015 using the Marketplace website (healthcare.gov), the health insurance companies' websites, and calls to insurance companies' customer service representatives. This information may change at any time and should be verified with the insurance company before enrolling in any plan. To calculate the cost of coinsurance, we used the Average Wholesale Price (AWP) of medications as listed in the 2014 Positively Aware HIV Drug Guide, which can be found here: Actual prices will vary between pharmacies and consumers should check with pharmacies before purchasing medications or selecting a plan that relies on coinsurance. Consumers should consider selecting a plan that requires a copay rather than coinsurance. A copay is a fixed and predictable amount of money and is typically considerably less than a coinsurance when applied to the costly medications used to treat HIV. More Information This document was originally prepared by Daliah Mehdi, Chief Clinical Officer, AIDS Foundation of Chicago; document was updated by Billy Minshall, Medical Benefits Coordinator, AIDS Foundation of Chicago. wminshall@aidschicago.org Plan Information Assurant Silver, Gold, and Platinum level plans from Assurant are compatible with Medication and Premium Assistance Programs. All Assurant 2015 Marketplace plans use either the 2 or 3 Tier formulary. Both formularies offer the same antiretrovirals at the same tier levels. The Assurant 2 Tier formulary can be accessed here: The Assurant 3 Tier formulary can be accessed here: Assurant designates its formulary tiers as follows.
4 Tier G P NP Description Generics Preferred brands Non-preferred brands Coverage of preferred regimen drugs (tiers P and NP) under each plan is outlined below. Note: Coverage under all plans only begins after deductible has been met. Until deductible is met, client pays full cost of medications. Plan Name Preferred brands Tier Non-Preferred Brand Tier Bronze Assurant Health Bronze Plan % covered 100% covered Assurant Health Bronze Plan % coinsurance 25% coinsurance Silver Assurant Health Silver Plan % covered 100% covered Assurant Health Silver Plan 002 $35 copay $60 copay Gold Assurant Health Gold Plan 002 $35 copay $60 copay Platinum Assurant Health Platinum Plan 002 $30 copay $50 copay The costs for components of preferred regimens when a 25% coinsurance is used are outlined in the following table. Medication Tier AWP 25% coinsurance Truvada preferred brand $1, $ Prezista preferred brand $1, $ Isentress non-preferred brand $1, $ Norvir preferred brand $ $77.15 Stribild non-preferred brand $2, $ Tivicay non-preferred brand $1, $ Epzicom non-preferred brand $1, $ Triumeq non-preferred brand $2,649 $ *Quantity Limits on all medications
5 Using the above costs, the calculated monthly cost for each preferred regimen is summarized below. Regimen Truvada + Prezista + Norvir Assurant Health Bronze Plan 001 Assurant Health Bronze Plan 002 Assurant Health Silver Plan 001 Assurant Health Silver Plan 002 Assurant Health Gold Plan 002 Assurant Health Platinum Plan 002 $ $105 $105 $90 Truvada + Isentress $ $95 $95 $80 Tivicay + Epzicom No cost after $6,000 $ No cost after $3,500 $120 $120 $100 Tivicay + Truvada deductible met $ deductible met $95 $95 $80 Stribild $ $60 $60 $50 Triumeq $ $60 $60 $50 Remember: A Silver, Gold or Platinum plan must be selected to qualify for Medication and Premium Assistance Program coverage of monthly premiums and out-of-pocket costs. Blue Cross Blue Shield of Illinois (BCBS) Silver, Gold, and Platinum level plans from BCBS are compatible with Medication and Premium Assistance Programs. All plans offered through the Marketplace use either the 2015 Standard Formulary or the 2015 Generics Plus Formulary. Both formularies offer the same antiretrovirals at the same tier levels. The Standard Formulary can be found here: The Generics Plus Formulary can be found here: BCBS designates its formulary tiers as follows. Tier Description 1 Preferred generic 2 Non-preferred generic 3 Preferred brand 4 Non-preferred brand 5 Specialty
6 The costs for components of preferred regimens are outlined in the following table. Standard/Generics Plus Formulary Medication Tier AWP All silver plans (except BCBS Solution 3, Multistate Plan), Blue Precision Gold HMO and Gold Multistate Plan All gold plans, (except Blue Precision Gold HMO and Gold Multistate Plan) and BCBS Solution 3, Multistate Plan Blue PPO Bronze 005 Bronze Blue Choice PPO 005 Bronze Multistate PPO Bronze Blue Precision HMO Truvada 3 $1, $50 $35 $ $ $ $ Prezista 3 $1, $50 $35 $ $ $ $ Isentress 3 $1, $50 $35 $ $ $ $ Norvir 3 $ $50 $35 $61.72 $61.72 $92.58 $ Tivicay 3 $1, $50 $35 $ $ $ $ Epzicom 3 $1, $50 $35 $ $ $ $ Stribild 3 $2, $50 $35 $ $ $ $ Triumeq 5 $2,649 $150 $150 $ $1, $ $1, *Dispensing Limits Note for Bronze Plans: Reflects prices after deductible is met Using the above costs, the calculated monthly cost for each preferred regimen is summarized below. Regimens Truvada + Prezista + Truvada + Isentress Tivicay + Epzicom Tivicay + Truvada All silver plans (except BCBS Solution 3, Multistate Plan), Blue Precision Gold HMO and Gold Multistate Plan All gold plans, (except Blue Precision Gold HMO and Gold Multistate Plan) and BCBS Solution 3, Multistate Plan Blue PPO Bronze 006 and Blue Choice Bronze 006 Plans Blue PPO Bronze 005 Bronze Blue Choice PPO 005 Bronze Multistate PPO Bronze Blue Precision HMO $150 $105 $0 $ $ $ $1, $100 $70 $0 $ $ $ $1, $100 $70 $0 $ $ $ $1, $100 $70 $0 $ $ $ $1, Stribild $50 $35 $0 $ $ $ $ Triumeq $150 $150 $0 $ $1, $ $1, Note for Bronze Plans: Reflects Prices after Deductible is Met Remember: A Silver, Gold or Platinum plan must be selected to qualify for Medication and Premium Assistance Program coverage of monthly premiums and out-of-pocket costs. Coventry Coventry plans are NOT compatible with Medication and Premium Assistance Programs.
7 * Coventry moved HIV medications to more affordable tiers effective June 1, This document has been updated to reflect those changes. The Coventry drug formulary can be found here: Coventry designates its formulary tiers as follows. Tier Description 1 Preferred generic and select over-the-counter drugs 2 Preferred brand drugs 3 Non-preferred generic and brand drugs 4 Specialty preferred 5 Specialty non-preferred Preferred regimen formulary tiers and restrictions. Medication Tier Notes Truvada 2 Prior Auth Prezista 3 Quant Limit Isentress 2 Quant Limit Norvir 3 Stribild 3 Prior Auth Tivicay 2 Epzicom 3 Prior Auth Triumeq not listed Cost of Preferred regimens according to tier per plan. Plan name Tier 2 Coverage Tier 3 Coverage Coventry Bronze $20 Copay Select $45 after $5,750 deductible $75 after $5,750 deductible Coventry Bronze Deductible Only HSA $0 after $6,300 deductible $0 after $6,300 deductible Eligible Select Coventry Silver $10 Copay Select $45 after $3,750 deductible $75 after $3,750 deductible Coventry Silver $5 Copay 2750 Select $45 after $2,750 deductible $75 after 2,750 deductible Coventry Gold $5 Copay Select $35 after $1,400 deductible $65 after 1,400 deductible
8 Using the table above, below are the costs of each preferred regimen per plan after deductible is met. Regimen Truvada + Prezista + Norvir Truvada + Isentress Coventry Bronze $20 Copay Select Coventry Bronze Deductible Only HSA Eligible Select Plan Coventry Silver $10 Copay Select Coventry Silver $5 Copay 2750 Select Coventry Gold $5 Copay Select $195 after deductible $0 after deductible $195 after deductible $195 after deductible $195 after deductible $90 after deductible $0 after deductible $90 after deductible $90 after deductible $70 after deductible Tivicay + Epzicom $120 after deductible $0 after deductible $120 after deductible $120 after deductible $100 after deductible Tivicay + Truvada $90 after deductible $0 after deductible $90 after deductible $90 after deductible $70 after deductible Stribild $75 after deductible $0 after deductible $75 after deductible $75 after deductible $65 after deductible Triumeq $2,649 $2,649 $2,649 $2,649 $2,649 Silver, Gold, and Platinum level plans from are compatible with Medication and Premium Assistance Programs. plans are available only outside the Chicago metro area. The formulary can be found here: designates its formulary tiers as follows. Tier Description 1 Generic 2 Preferred brand drugs 3 Non-preferred brand drugs 4 Preferred specialty drugs 5 Non-preferred specialty drugs 6 Non-formulary specialty drugs The costs for components of preferred regimens are outlined in the following table. Medication Tier AWP* 20% coinsurance 30% coinsurance 45% Coinsurance 50% coinsurance Truvada 5 $1, $ $ $ $ Prezista 3 $1, $ $ $ $ Isentress 2 $1, $ $ $ $ Norvir 2 $ $61.72 $92.58 $ $ Tivicay 5 $1, $ $ $ $ Epzicom 2 $1, $ $ $ $ Stribild 5 $2, $ $ $1, $1, Triumeq 5 $2, $ $ $1, $1,324.50
9 Coverage of preferred regimen drugs (tiers 3 and 5) under each plan is outlined below. Plan Tier 2 (preferred brand) Coverage Tier 3(non-preferred brand) Coverage Tier 5(non-preferred specialty) Coverage HMO 4000b Silver, HMO 1500a Gold, 1500b Gold, and HMO 2750 Gold $25 $50 $150 HMO HSA 3000 Bronze, HMO 5000c Silver & PPO 4500b Silver POS 5000a Bronze 20% coinsurance 20% coinsurance 20% coinsurance POS HSA 3750a Bronze 30% coinsurance 30% coinsurance 30% coinsurance HMO 4000D Bronze & POS 4000a Bronze 50% coinsurance 50% coinsurance 50% coinsurance POS HSA 3750c Bronze 45% coinsurance 45% coinsurance 45% coinsurance POS HAS 2000 Gold & POS HAS 2100a Gold $0 after deductible $0 after deductible $0 after deductible PPO 2000 Gold $25 $50 $150 PP Silver, PPO 3250b Gold& POS 6000b Silver $35 $70 $210 Using the above costs, the calculated monthly cost for each preferred regimen is summarized below. Cost per month of preferred regimens by plan HMO 4000b Silver, HMO 1500a Gold, HMO 1500b Gold, and Health Alliance HMO 2750 Gold HMO HSA 3000 Bronze, Health Alliance HMO 5000c Silver & PPO 4500b Silver POS 5000a Bronze POS HSA 3750a Bronze HMO 4000D Bronze & POS 4000a Bronze POS HSA 3750c Bronze POS HSA 2000 Gold & POS HSA 2100a Gold PPO 2000 Gold PP Silver, PPO 3250b Gold& POS 6000b Silver Truvada + Prezista + Norvir $225 $420 $ $ $1, $1, $0 $225 $315 Truvada + Isentress $175 $340 $ $ $1, $1, $0 $175 $245 Tivicay + Epzicom $175 $340 $ $ $1, $1, $0 $175 $245 Tivicay + Truvada $300 $600 $ $ $1, $1, $0 $300 $420 Stribild $150 $300 $ $ $1, $1, $0 $150 $210 Triumeq $150 $300 $ $ $1, $1, $0 $150 $210 Benefits begin after deductible met Remember: A Silver, Gold or Platinum plan must be selected to qualify for Medication and Premium Assistance Program coverage of monthly premiums and out-of-pocket costs. Humana Humana plans are NOT compatible with Medication and Premium Assistance Programs. All marketplace plans use either the Rx5 Plus formulary or the HDHP Plus formulary. All of the medications in the preferred regimens are listed as Tier 5 in both formularies. The Rx5 Plus formulary can be found here: The HDHP Plus formulary can be found here: Humana designates its formulary tiers as follows. Tier Description 1 Preferred generic 2 Non-preferred generic
10 3 Preferred brand 4 Non-preferred brand 5 Specialty Note that all of the high deductible health plans (HDHPs) use the HDHP Plus formulary. Under these plans there is no cost to the client for medications once the deductible has been met. Until the deductible is met the patient is responsible for 100% of the cost of the medication. The coverage for each Humana plan offered is in the following table. Plan type Plan name Tier 5 coverage HMO Humana Bronze 6300/Chicago HMOx 100% after deductible Humana Bronze 4850/Chicago HMOx Humana Silver 4600/Chicago HMOx Humana Gold 2500/Chicago HMOx Humana Platinum 1000/Chicago HMOx 50% coinsurance after deductible 50% coinsurance after deductible 35% coinsurance after deductible 35% coinsurance after deductible PPO Humana Bronze 4850/Choice POS 50% coinsurance after deductible Humana Silver 4250/Choice POS Humana Silver 3650/Choice POS Humana Gold 2500/Choice POS Humana Bronze 6300/Choice POS 50% coinsurance after deductible 100% after deductible 35% coinsurance after deductible 100% after deductible The costs for components of preferred regimens are outlined in the following table. Medication Tier AWP 35% Coinsurance 50% Coinsurance Truvada 5 $1, $ $ Prezista 5 $1, $ $ Isentress 5 $1, $ $ Norvir 5 $ $ $ Tivicay 5 $1, $ $ Epzicom 5 $1, $ $ Stribild 5 $2, $1, $1, Triumeq 5 $2, $ $1, * Dispensing Limits for all meds Using the above costs, the calculated monthly cost for each preferred regimen is summarized below.
11 35% coinsurance 50% coinsurance Truvada + Prezista + Norvir $1, $1, Truvada + Isentress $1, $1, Tivicay + Epzicom $ $1, Tivicay + Truvada $1, $1, Stribild $1, $1, Triumeq $ $1, IlliniCare IlliniCare plans are NOT compatible with Medication and Premium Assistance Programs. The IlliniCare drug formulary can be found here: IlliniCare designates its formulary tiers as follows. Tier Description 0 Preventative 1 Generic 2 Preferred 3 Non-preferred 4 Specialty Coverage of preferred regimen drugs (tiers 2 and 3) under each plan is outlined below. Metal Level Plan Tier 2 Coverage Tier 3 Coverage Deductible Essential Care 1 100% after deductible 100% after deductible $6,500 Bronze Essential Care 2 $50 after deductible $100 after deductible $5,000 Essential Care 3 $50 after deductible $100 after deductible $6,000 Essential Care 4 $100 after deductible $150 after deductible $4,000 Balanced Care 1 $60 after deductible 50% after deductible $750 Silver Balanced Care 2 $50 copay 100% after deductible $5,000 Balanced Care 3 $50 after deductible $100 after deductible $1,000 Balanced Care 4 $50 copay $100 after deductible $2,000 Gold Secure Care 1 $25 after deductible $75 after deductible $500 Secure Care 2 $30 after deductible $100 after deductible $500 Platinum Platinum Care 1 $40 after deductible 30% after deductible $250
12 The costs for components of preferred regimens are outlined in the following table. Medication AWP Tier 30% coinsurance 50% coinsurance Truvada $1, $ $ Prezista $1, $ $ Isentress $1, $ $ Norvir $ $92.58 $ Tivicay $1, not covered not covered not covered Epzicom $1, $ $ Stribild $2, not covered not covered not covered Triumeq $2, not covered not covered not covered Using the above costs, the calculated monthly cost for each preferred regimen is summarized below. Essential Care 1 Essential Care 2 Bronze Silver Gold Essential Care 3 Essential Care 4 Balanced Care 1 Balanced Care 2 Balanced Care3 Balanced Care 4 Secure Care 1 Secure Care 2 Platinum Platinum Care 1 Truvada + Prezista + Norvir $0 $150 $150 $300 $180 $150 $150 $150 $75 $90 $120 Truvada + Isentress $0 $100 $100 $200 $120 $100 $200 $100 $50 $60 $80 Tivicay + Epzicom $1, $1,530 $1,530 $1, $1,540 $1, $1,530 $1, $1,505 $1,510 $1,520 Tivicay + Truvada $1, $1,530 $1,530 $1, $1,540 $1, $1,530 $1, $1,505 $1,510 $1,520 Stribild $2, $2, $2, $2, $2, $2, $2, $2, $2, $2, $2, Triumeq $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 $2,649 Deductible $6,500 $5,000 $6,000 $4,000 $750 $5,000 $1,000 $2,000 $500 $500 $250 Seperate or Combined Combined Combined Combined Combined Separate Combined Separate Combined Separate Separate Separate Land of Lincoln Land of Lincoln plans are NOT compatible with Medication and Premium Assistance Programs. Updates made 3/25/2015. The Land of Lincoln formulary can be found here: Land of Lincoln designates its formulary tiers as follows. Tier Description 1 Generic 2 Preferred brand drugs 3 Non-preferred brand drugs 4 Specialty drugs The costs for components of preferred regimens are outlined in the following table. Medication Tier AWP 10% coinsurance 20% coinsurance 25% coinsurance 30% coinsurance 35% coinsurance 40% coinsurance Truvada 2 $1, $ $ $ $ $ $ Prezista 2 $1, $ $ $ $ $ $ Isentress 2 $1, $ $ $ $ $ $ Norvir 2 $ $30.86 $61.72 $77.15 $92.58 $ $ Tivicay 4 $1, $ $ $ $ $ $ Epzicom 2 $1, $ $ $ $ $ $ Stribild 2 $2, $ $ $ $ $1, $1, Triumeq Not Covered $2,649 $ $ $ $ $ $1,059.60


13 Using the above costs, the calculated monthly cost for each preferred regimen is summarized below.
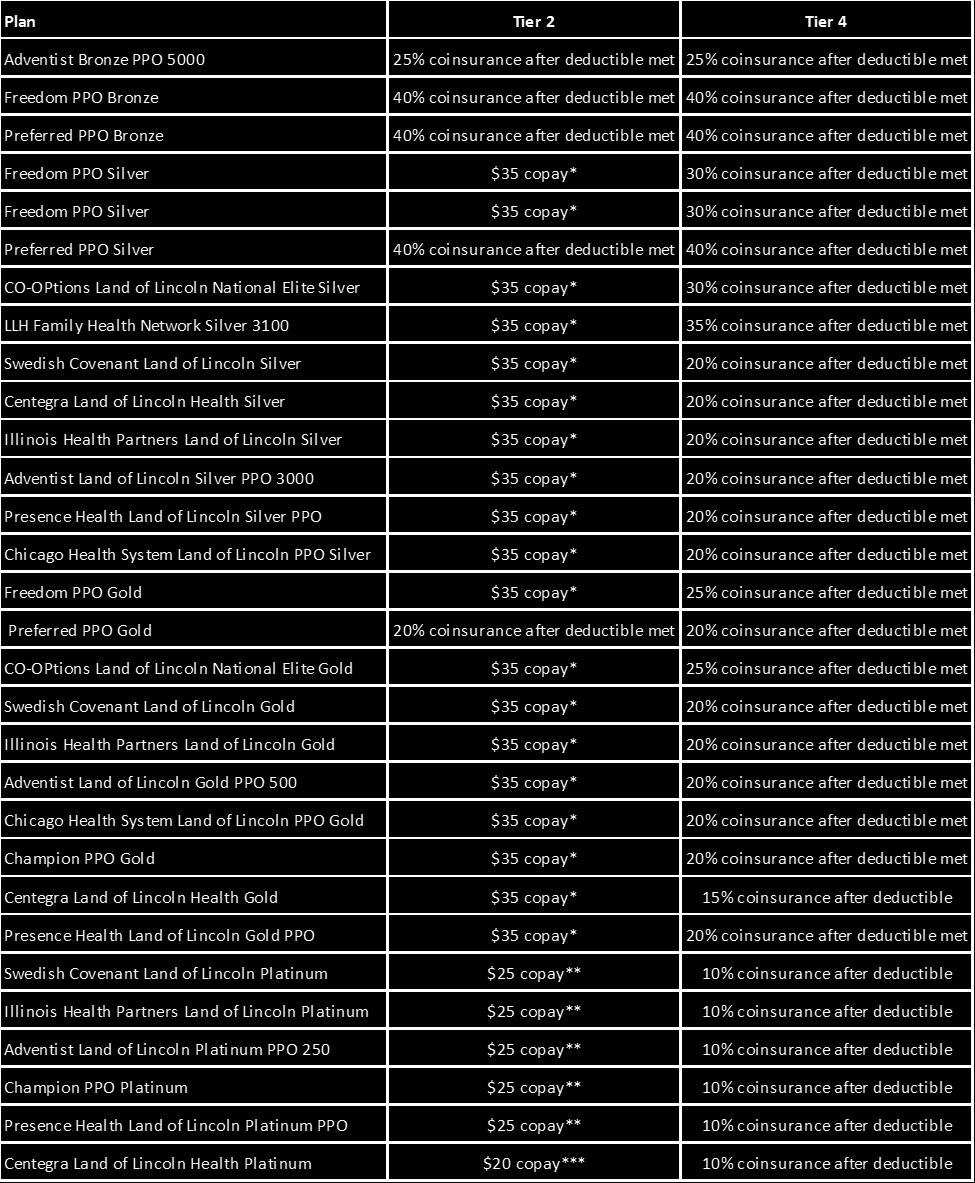
14
15 Plans from are NOT compatible with Medication and Premium Assistance Programs. Updates as of 3/25/2015. The formulary can be found here: DL.pdf designates its formulary tiers as follows. Tier Description 1 Generic 2 Preferred brand drugs 3 Non-preferred brand drugs 4 Specialty drugs Coverage of preferred regimen drugs under each plan is outlined below. Note: Coverage under all plans only begins after deductible has been met. Until deductible is met, client pays full cost of medications. Medication Tier specialty notification AWP 30% coinsurance 20% coinsurance Truvada 2 yes yes $1, $ $ Prezista 2 yes $1, $ $ Isentress 2 yes $1, $ $ Norvir 2 yes $ $92.58 $61.72 Stribild 4 yes yes $2, $ $ Tivicay 4 yes $1, $ $ Epzicom 2 yes $1, $ $ Triumeq 3 Yes $2,649 $ $529.80
16 Using the above costs, the calculated monthly cost for each preferred regimen is summarized below. Note: Coverage under all plans only begins after deductible has been met. Until deductible is met, client pays full cost of medications. Regimen Truvada + Prezista + Norvir Bronze Compass HSA 4900 Bronze Plans Silver Plans Gold Plans Bronze Compass 5500 Silver Compass HSA 2600 Silver Compass 2000 Silver Compass 3500 Silver Compass 5000 Silver Compass HSA 1600 Gold Compass 500 Gold Compass 1250 Platinum Plans Platinum Compass 250 $ $ $ $ $ $ $ $ $ $ Truvada + Isentress $ $ $80.00 $ $90.00 $ $ $80.00 $80.00 $70.00 Tivicay + Epzicom $ $ $ $ $ $ $ $ $ $ Tivicay + Truvada $ $ $ $ $ $ $ $ $ $ Stribild $ $ $ $ $ $ $ $ $ $ Triumeq $ $ $ $ $ $ $ $ $ $529.80
Humana medical plans For groups 1 50 (includes pediatric dental and vision) Effective dates starting 1/1/17
 Effective dates starting 1/1/17") Humana medical plans For groups 1 50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups 1 50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17
 Effective dates starting 1/1/17") Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Florida Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Florida Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17
 Effective dates starting 1/1/17") Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Kentucky Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups 1-50 (includes pediatric dental and vision) Effective dates starting 1/1/17 Kentucky Humana s benefit plans help your employees get and stay well so your business can flourish.
Humana medical plans For groups Effective dates starting 1/1/17
 Humana medical plans For groups 51-100 Effective dates starting 1/1/17 Kentucky Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
Humana medical plans For groups 51-100 Effective dates starting 1/1/17 Kentucky Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
Humana medical plans For groups Effective dates starting 1/1/17
 Humana medical plans For groups 51 100 Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
Humana medical plans For groups 51 100 Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
Estimated monthly premium. Deductible. Choose a maximum yearly deductible. $100 $1000+ Medical management programs
 Choose a maximum yearly deductible. $100 $1000+ Medical management programs Select any program a plan must offer. Select a medical management program Insurance Companies Select an insurance company to
Choose a maximum yearly deductible. $100 $1000+ Medical management programs Select any program a plan must offer. Select a medical management program Insurance Companies Select an insurance company to
Humana medical plans For groups Effective dates starting 1/1/17
 Humana medical plans For groups 51-100 Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
Humana medical plans For groups 51-100 Effective dates starting 1/1/17 Illinois Humana s benefit plans help your employees get and stay well so your business can flourish. You and your business receive:
BlueCross BlueShield of North Carolina: Blue Value Bronze 5500 (limited network, HSA eligible)
") BlueCross BlueShield of North Carolina: Blue Value Bronze 5500 (limited network, HSA eligible) $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers &
BlueCross BlueShield of North Carolina: Blue Value Bronze 5500 (limited network, HSA eligible) $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers &
BlueCross BlueShield of North Carolina: Blue Local Silver 3000 (local network with Carolinas HealthCare System)
") BlueCross BlueShield of North Carolina: Blue Local Silver 3000 (local network with Carolinas HealthCare System) $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this
BlueCross BlueShield of North Carolina: Blue Local Silver 3000 (local network with Carolinas HealthCare System) $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this
Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Silver Plan Coverage Period: Beginning on or after 01/01/2014
 Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: Beginning on or after 01/01/2014 Coverage
Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Silver Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: Beginning on or after 01/01/2014 Coverage
2019 MEDICARE. summary of benefits. advantage plan. Serving Members in Douglas County
 2019 MEDICARE advantage plan summary of benefits Serving Members in Douglas County Table of Contents About the Summary of Benefits and Who Can Join... 1 Which doctors, hospitals and pharmacies can I use?...
2019 MEDICARE advantage plan summary of benefits Serving Members in Douglas County Table of Contents About the Summary of Benefits and Who Can Join... 1 Which doctors, hospitals and pharmacies can I use?...
BlueCross BlueShield of North Carolina: Blue Cross Blue Shield 200, a Multi-State Plan
 BlueCross BlueShield of North Carolina: Blue Cross Blue Shield 200, a Multi-State Plan $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
BlueCross BlueShield of North Carolina: Blue Cross Blue Shield 200, a Multi-State Plan $$start$$ Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it
CIS - Copay Plan A RX4 with Hearing Aids Coverage Period: 01/01/ /31/2016
 CIS - Copay Plan A RX4 with Hearing Aids Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual & Eligible Family Plan Type:
CIS - Copay Plan A RX4 with Hearing Aids Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual & Eligible Family Plan Type:
BlueCross BlueShield of North Carolina: Blue Advantage Silver 2800
 BlueCross BlueShield of North Carolina: Blue Advantage Silver 2800 $$start$$ Coverage Period: 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
BlueCross BlueShield of North Carolina: Blue Advantage Silver 2800 $$start$$ Coverage Period: 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
ID Prefix XQW RDP RDP Annual Enrollment
 ID Prefix XQW RDP RDP Annual Enrollment Employees who are not currently enrolled in a MIIP Employees who are not currently enrolled in a MIIP health insurance plan can NOT come on to this plan at health
ID Prefix XQW RDP RDP Annual Enrollment Employees who are not currently enrolled in a MIIP Employees who are not currently enrolled in a MIIP health insurance plan can NOT come on to this plan at health
You don't have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
 SBC0120W100620161609 HUMANA INSURANCE COMPANY: CR HUMANA PPO EHDHP 17 DED/COINS OV,IP,OP Coverage Period: Beginning on or after 01/01/2017 Summary of Benefits and Coverage: What this Plan Covers & What
SBC0120W100620161609 HUMANA INSURANCE COMPANY: CR HUMANA PPO EHDHP 17 DED/COINS OV,IP,OP Coverage Period: Beginning on or after 01/01/2017 Summary of Benefits and Coverage: What this Plan Covers & What
Highmark Health Insurance Company: Alliance Flex Blue PPO 1000 ONX (Base Plan)
") This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-888-510-1064.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkblueshield.com or by calling 1-888-510-1064.
Blue Cross Blue Shield Blue Options ~ HSA (Health Savings Account)
") Blue Cross Blue Shield Blue Options ~ HSA (Health Savings Account) The Health Savings Account (HSA) is established by Robeson County Government. The HSA is administered by Mellon Financial Corporation
Blue Cross Blue Shield Blue Options ~ HSA (Health Savings Account) The Health Savings Account (HSA) is established by Robeson County Government. The HSA is administered by Mellon Financial Corporation
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-451-1527. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-451-1527. Important Questions
40 SimpleCare plans offered in 2017 for small group clients. All 40 plans are available OFF The Health Insurance Marketplace (SHOP)
") Products available both ON and OFF The Health Insurance Marketplace 40 Simple plans offered in for small group clients. All 40 plans are available OFF The Health Insurance Marketplace (SHOP) 17 plans available
Products available both ON and OFF The Health Insurance Marketplace 40 Simple plans offered in for small group clients. All 40 plans are available OFF The Health Insurance Marketplace (SHOP) 17 plans available
Regence Copay Plan A Coverage Period: 01/01/ /31/2017
 Regence Copay Plan A Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017-12/31/2017 Coverage for: Individual & Eligible Family Plan Type: PPO This is only
Regence Copay Plan A Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2017-12/31/2017 Coverage for: Individual & Eligible Family Plan Type: PPO This is only
Important Questions Answers Why this Matters:
 Anthem BlueCross BlueShield Blue Access Choice PPO Option 16 / Rx Option AJ Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2014-06/30/2015 Coverage For:
Anthem BlueCross BlueShield Blue Access Choice PPO Option 16 / Rx Option AJ Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2014-06/30/2015 Coverage For:
Maine's Choice Pemaquid Silver HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Maine Maine's Choice Pemaquid Silver HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family
Maine Maine's Choice Pemaquid Silver HMO Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Coverage for: Individual + Family
HEALTH PLAN BENEFIT SUMMARIES
 HEALTH PLAN BENEFIT SUMMARIES Kaiser Permanente Small Business Group Plans effective April 2012 The Small Group Endura SM portfolio affordable and adaptable. Coverage from a partner you trust. With our
HEALTH PLAN BENEFIT SUMMARIES Kaiser Permanente Small Business Group Plans effective April 2012 The Small Group Endura SM portfolio affordable and adaptable. Coverage from a partner you trust. With our
BlueCross BlueShield of North Carolina: Blue Options Coverage Period: 07/01/ /30/2015
 $$start$$ BlueCross BlueShield of North Carolina: Blue Options Coverage Period: 07/01/2014-06/30/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual +
$$start$$ BlueCross BlueShield of North Carolina: Blue Options Coverage Period: 07/01/2014-06/30/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual +
Regence BlueCross BlueShield of Oregon: Preferred Coverage Period: 01/01/ /31/2016
 Regence BlueCross BlueShield of Oregon: Preferred Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual & Eligible Family
Regence BlueCross BlueShield of Oregon: Preferred Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 12/31/2016 Coverage for: Individual & Eligible Family
HUMANA INSURANCE COMPANY:
 HUMANA INSURANCE COMPANY: Humana Local Preferred Silver 4600/6300 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HUMANA INSURANCE COMPANY: Humana Local Preferred Silver 4600/6300 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HUMANA INSURANCE Humana National Preferred Silver 4250/6250 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage:
 HUMANA INSURANCE Humana National Preferred Silver 4250/6250 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
HUMANA INSURANCE Humana National Preferred Silver 4250/6250 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
Important Questions Answers Why this Matters:
 Anthem Blue Cross: Anthem Preferred DirectAccess - ccas Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual / Family
Anthem Blue Cross: Anthem Preferred DirectAccess - ccas Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual / Family
Small Group Benefit Comparison
 Small Group Benefit Comparison effective January 1, 2015 A guide to choosing the right plan for your business We re Proud to Be a Top 100 Health Plan 1 At Sharp Health Plan, we believe in making life better.
Small Group Benefit Comparison effective January 1, 2015 A guide to choosing the right plan for your business We re Proud to Be a Top 100 Health Plan 1 At Sharp Health Plan, we believe in making life better.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan
 Vincennes University: Blue Access (PPO) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This
Vincennes University: Blue Access (PPO) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This
Medtronic HRA Plan Coverage Period: Beginning on or after
 Medtronic HRA Plan Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage Period: Beginning on or after 01-01-2016 Coverage for: All Coverage Levels Plan Type: HDHP This is only
Medtronic HRA Plan Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage Period: Beginning on or after 01-01-2016 Coverage for: All Coverage Levels Plan Type: HDHP This is only
Important Questions Answers. Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-800-227-3641. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-800-227-3641. Important
Important Questions Answers Why this Matters:
 CEBCO: Union County Modified Plan 2 Blue Access (PPO) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
CEBCO: Union County Modified Plan 2 Blue Access (PPO) Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
HEALTH PLAN BENEFIT SUMMARIES
 KAISER PERMANENTE SMALL BUSINESS GROUP HEALTH PLAN BENEFIT SUMMARIES 1 The Colorado Division of Insurance may amend copayments, coinsurance and/or s. Please contact your broker or Kaiser Permanente sales
KAISER PERMANENTE SMALL BUSINESS GROUP HEALTH PLAN BENEFIT SUMMARIES 1 The Colorado Division of Insurance may amend copayments, coinsurance and/or s. Please contact your broker or Kaiser Permanente sales
limit. The chart starting on page 2 describes any limits on what the plan will pay for specific covered services, such as office visits.
 Medtronic BCBSMN PPO Plan Coverage Period: Beginning on or after 01-01-2016 Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage for: Single and family coverage Plan Type: PPO
Medtronic BCBSMN PPO Plan Coverage Period: Beginning on or after 01-01-2016 Summary of Benefits and Coverage: What this Plan covers & What it Costs Coverage for: Single and family coverage Plan Type: PPO
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Highmark Blue Cross Blue Shield: Community Blue PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 10/01/2018-09/30/2019 Highmark Blue Cross Blue Shield: Community Blue PPO Coverage for: Individual/Family
PPO 100+ Product Coverage Options. Accounts with 100 or more Eligible Employees. Effective on anniversary dates on or after January 2018
 Product Coverage Options PPO 100+ Accounts with 100 or more Eligible Employees Effective on anniversary dates on or after January 2018 Blue Cross Blue Shield of Massachusetts covers more people in Massachusetts
Product Coverage Options PPO 100+ Accounts with 100 or more Eligible Employees Effective on anniversary dates on or after January 2018 Blue Cross Blue Shield of Massachusetts covers more people in Massachusetts
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: HDHP PPO Blue Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: HDHP PPO Blue Coverage for: Individual/Family
Important Questions. Why this Matters:
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Member Only Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you can get
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Member Only Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you can get
WPAHS: Community Blue HDHP Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at Highmarkbcbs.com or by calling 1-800-472-1506. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at Highmarkbcbs.com or by calling 1-800-472-1506. Important
EBC Board of Education #83: PPO Plan Coverage Period: 07/01/ /30/2017
 EBC Board of Education #83: PPO Plan Coverage Period: 07/01/2016-06/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This
EBC Board of Education #83: PPO Plan Coverage Period: 07/01/2016-06/30/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: PPO This
Educators Health Alliance Coverage Period: 09/01/ /31/2017
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more detail about
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more detail about
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Regence BlueCross BlueShield of Oregon: Preferred Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Regence BlueCross BlueShield of Oregon: Preferred Coverage for: Individual
Healthy Benefits PPO HSA STD
 Healthy Benefits PPO HSA 3000.10 STD Coverage Period: Beginning on or after 1/1/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the
Healthy Benefits PPO HSA 3000.10 STD Coverage Period: Beginning on or after 1/1/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the
Coverage Period: 01/01/ /31/2019 A nonprofit independent licensee of the BlueCross BlueShield Association
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: SimplyBlue Plus Platinum 2 Coverage Period: 01/01/2019-12/31/2019 A nonprofit independent licensee
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Excellus BCBS: SimplyBlue Plus Platinum 2 Coverage Period: 01/01/2019-12/31/2019 A nonprofit independent licensee
Summary of Benefits and Coverage:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018-06/30/2019 Allegheny County Schools Health Insurance Consortium: Community Blue Flex
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2018-06/30/2019 Allegheny County Schools Health Insurance Consortium: Community Blue Flex
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket
 Regence BlueCross BlueShield of Utah: Regence BluePoint Coverage Period: 04/01/2016 03/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible
Regence BlueCross BlueShield of Utah: Regence BluePoint Coverage Period: 04/01/2016 03/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible
Important Questions Answers Why this Matters:
 Regence BlueShield: Regence EmployeeChoice Platinum 250 Coverage Period: [When enrolled, the coverage period will show here] Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Regence BlueShield: Regence EmployeeChoice Platinum 250 Coverage Period: [When enrolled, the coverage period will show here] Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Roosevelt University Student Health Insurance Plan. Dear Student:
 Roosevelt University Student Health Insurance Plan Dear Student: Under the Affordable Care Act, all health insurers and group health plans are required to provide consumers with a Summary of Benefits and
Roosevelt University Student Health Insurance Plan Dear Student: Under the Affordable Care Act, all health insurers and group health plans are required to provide consumers with a Summary of Benefits and
2019 Staff Medical Plan Options
 2019 Staff Medical Plan Options PHBP Staff Plan Options: PHBP Classic Premier PPO PHBP Classic Plus PPO PHBP California Classic HMO (CA Only) PHBP Health Savings Account (HSA) Anthem Plan Designations
2019 Staff Medical Plan Options PHBP Staff Plan Options: PHBP Classic Premier PPO PHBP Classic Plus PPO PHBP California Classic HMO (CA Only) PHBP Health Savings Account (HSA) Anthem Plan Designations
$750 individual/$1,500 family enhanced value network. $2,250 individual/$4,500 family standard value network.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Journey Health System: Community Blue Flex PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Journey Health System: Community Blue Flex PPO Coverage for: Individual/Family
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-333-5730. Important
Even though you pay these expenses, they don t count toward the out-ofpocket limit.
 Ohio Northern University: Blue Access (PPO) $500 Plan A Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
Ohio Northern University: Blue Access (PPO) $500 Plan A Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan
HUMANA INSURANCE COMPANY:
 HUMANA INSURANCE COMPANY: Humana Local Preferred Silver 4600/6300 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HUMANA INSURANCE COMPANY: Humana Local Preferred Silver 4600/6300 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
PLATINUM GOLD SILVER BRONZE VANTAGE HEALTH PLAN HEALTH INSURANCE MARKETPLACE PLAN FINDER HEALTH PLAN
 PLATINUM GOLD SILVER BRONZE VANTAGE HEALTH PLAN HEALTH INSURANCE MARKETPLACE PLAN FINDER HEALTH PLAN PICK YOUR PLAN Thanks, Vantage, for making it so easy! Vantage Platinum No deductibles and lowest copay
PLATINUM GOLD SILVER BRONZE VANTAGE HEALTH PLAN HEALTH INSURANCE MARKETPLACE PLAN FINDER HEALTH PLAN PICK YOUR PLAN Thanks, Vantage, for making it so easy! Vantage Platinum No deductibles and lowest copay
Best Buy HSA PPO FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
 Massachusetts Best Buy HSA PPO 3100 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018 03/31/2019 Coverage for: Individual +
Massachusetts Best Buy HSA PPO 3100 - FLEX Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 04/01/2018 03/31/2019 Coverage for: Individual +
COLGATE UNIVERSITY - Active Excellus BCBS: Excellus BluePPO
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services COLGATE UNIVERSITY - Active Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services COLGATE UNIVERSITY - Active Excellus BCBS: Excellus BluePPO Coverage Period: 01/01/2019-12/31/2019 A nonprofit
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 WRC Senior Services: PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 WRC Senior Services: PPO Coverage for: Individual/Family Plan Type: PPO
$300 individual/$900 family network. $1,200 individual/$3,600 family out-ofnetwork.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
NC Medical Society: HDHP
 NC Medical Society: HDHP 3500-100 $$start$$ Coverage Period: 08/01/2014-07/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
NC Medical Society: HDHP 3500-100 $$start$$ Coverage Period: 08/01/2014-07/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
CUSD #300 PPO Plus: Blue Cross and Blue Shield of Illinois Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 Coverage Period: 01/01/2016-12/31/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsil.com or
Coverage Period: 01/01/2016-12/31/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsil.com or
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 Highmark Blue Shield: PPO Coverage for: Individual/Family Plan Type: PPO
Important Questions Answers Why this Matters: In-network: $200/Individual; $400/Family Out-of-network: $1,000/Individual; $2,000/Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-800-451-1527.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso or by calling 1-800-451-1527.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-542-9402. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-542-9402. Important Questions
Palmetto Health : HRA Medical Tuomey
 Palmetto Health : HRA Medical Tuomey Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual Plan Type: 3 Tier PPO This is
Palmetto Health : HRA Medical Tuomey Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016-12/31/2016 Coverage for: Individual Plan Type: 3 Tier PPO This is
The out-of-pocket limit is the most you could pay during a coverage period. Coinsurance and copayments do. In-Network preventive care.
 $$start$$ Rowan County Government: GOV Plan Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
$$start$$ Rowan County Government: GOV Plan Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
NC Medical Society: HDHP
 NC Medical Society: HDHP 2700-100 $$start$$ Coverage Period: 01/01/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
NC Medical Society: HDHP 2700-100 $$start$$ Coverage Period: 01/01/2017-12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-852-9995. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-855-852-9995. Important
Highmark Blue Cross Blue Shield: BLUECARE CUSTOM PPO EXP Coverage Period: 01/01/ /31/2017
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Highmark Blue Shield: PPO Coverage Period: 07/01/2017-06/30/2018 Coverage for: Individual/Family Plan Type: PPO The Summary of Benefits
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Highmark Blue Shield: PPO Coverage Period: 07/01/2017-06/30/2018 Coverage for: Individual/Family Plan Type: PPO The Summary of Benefits
You don t have to meet deductibles for specific services. 1 of 10 *Precertification may be required GE_ _ _SBC
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018-12/31/2018 Highmark Blue Cross Blue Shield: BlueCare Custom PPO Coverage for: Individual/Family
Important Questions Answers Why this Matters: In-network: $500/Individual; $1,000/Family Out-of-network:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-445-7490. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-445-7490. Important Questions
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services. Coverage Period: 1/1/ /31/2018
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 12/31/2018 County of Orange Wellwise Choice Coverage for: Individual + Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2018 12/31/2018 County of Orange Wellwise Choice Coverage for: Individual + Family Plan
Assurant Health. Time Insurance Company. Summary of Benefits and Coverage for Assurant Health individual major medical Platinum plans
 Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Platinum plans View Summary of Benefits and Coverage for an individual plan View Summary
Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Platinum plans View Summary of Benefits and Coverage for an individual plan View Summary
Cummins Central Power, LLC Coverage Period: 05/01/ /30/2016
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more detail about
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more detail about
Assurant Health Silver Plan 002: Time Ins. Co. Coverage Period: 01/01/ /31/2015 Summary of Benefits and Coverage:
 Assurant Health Silver Plan 002: Time Ins. Co. Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Family Plan Type: PPO This is
Assurant Health Silver Plan 002: Time Ins. Co. Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Family Plan Type: PPO This is
Premium, balance-billed charges, and health care this plan doesn't cover.
 Assurant Health Silver Plan 002: Time Ins. Co. Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Family Plan Type: PPO This is
Assurant Health Silver Plan 002: Time Ins. Co. Coverage Period: 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Family Plan Type: PPO This is
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket
 Regence BlueCross BlueShield of Oregon: Preferred Coverage Period: 12/01/2014-11/30/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible Family
Regence BlueCross BlueShield of Oregon: Preferred Coverage Period: 12/01/2014-11/30/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible Family
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: Affordablue $500/$1500/$4000 Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Cross Blue Shield: Affordablue $500/$1500/$4000 Coverage
You don t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
 Blue Care Elect Preferred 80 Copay Le Cordon Bleu Students Coverage Period: 2016-2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type:
Blue Care Elect Preferred 80 Copay Le Cordon Bleu Students Coverage Period: 2016-2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type:
starting on page 2 for how much you pay for covered services after you meet the
 Columbus County: BO 123 Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This is only a summary.
Columbus County: BO 123 Coverage Period: 07/01/2015-06/30/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This is only a summary.
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 08/01/2018-07/31/2019 Highmark Blue Cross Blue Shield: PPO Coverage for: Individual/Family Plan
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 08/01/2018-07/31/2019 Highmark Blue Cross Blue Shield: PPO Coverage for: Individual/Family Plan
Anthem Blue Cross and Blue Shield East Central College Blue Access Choice PPO and Blue Preferred Select - Base Plan
 plan pays different kinds of providers. This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or
plan pays different kinds of providers. This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or
NC Medical Society: HDHP
 NC Medical Society: HDHP 6350-100 $$start$$ Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
NC Medical Society: HDHP 6350-100 $$start$$ Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO
CHOOSE A PLAN CHOOSE A PLAN
 CHOOSE A PLAN CHOOSE A PLAN Choose from 17 plans, including copayment, deductible, and deductible plans that are compatible with a health savings account (HSA). IN THIS BROCHURE n Traditional copayment
CHOOSE A PLAN CHOOSE A PLAN Choose from 17 plans, including copayment, deductible, and deductible plans that are compatible with a health savings account (HSA). IN THIS BROCHURE n Traditional copayment
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Health Insurance Company: Shared Cost Blue PPO Bronze 7500 Coverage
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Health Insurance Company: Shared Cost Blue PPO Bronze 7500 Coverage
01/01/ /31/2018 UMR: COLE COUNTY COMMISSION:
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 UMR: COLE COUNTY COMMISSION: 7670-00-411637 001 Coverage for: Individual
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2018 12/31/2018 UMR: COLE COUNTY COMMISSION: 7670-00-411637 001 Coverage for: Individual
Aetna Choice POS II (HDHP) Coverage Period: 01/01/ /31/2014
 Coverage Period: 01/01/ /31/2014") This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-888-982-3862.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-888-982-3862.
1 of 10 *Precertification may be required G_ _ _SBC
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2017-06/30/2018 LCIC Penn College of Technology: QHDHP PPO Coverage for: Individual/Family Plan Type: PPO
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 07/01/2017-06/30/2018 LCIC Penn College of Technology: QHDHP PPO Coverage for: Individual/Family Plan Type: PPO
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthscopebenefits.com or by calling 1-877-385-8816.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthscopebenefits.com or by calling 1-877-385-8816.
Assurant Health. Time Insurance Company. Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans
 Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
Important Questions Answers Why this Matters: For in-network providers AND out-of-network providers combined: $1,750 Individual; $4,250 Family
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso by calling 1-800-582-6941.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://eoc.anthem.com/eocdps/aso by calling 1-800-582-6941.
In-Network Providers $1,400 per employee $2,800 per employee & spouse $2,800 per employee & child(ren) $3,600 per family
 $3,600 per family") Medtronic Consumer Health Plan (CHP) with HSA (Health Savings Account) Coverage Period: Beginning on or after 1/1/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
Medtronic Consumer Health Plan (CHP) with HSA (Health Savings Account) Coverage Period: Beginning on or after 1/1/2018 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered
HUMANA HEALTH PLAN, INC.: KY LG CF Coverage Period: 01/01/ /31/2016 Maximum Out-of-Pocket Explanation. Special Notice:
 HUMANA HEALTH PLAN, INC.: KY LG CF Coverage Period: 01/01/2016-12/31/2016 Maximum Out-of-Pocket Explanation Plan Type: CF Copay Special Notice: Starting in 2014 there will be a federally mandated maximum
HUMANA HEALTH PLAN, INC.: KY LG CF Coverage Period: 01/01/2016-12/31/2016 Maximum Out-of-Pocket Explanation Plan Type: CF Copay Special Notice: Starting in 2014 there will be a federally mandated maximum
Lumenos HK HDHP: Henrico County General Government and and Public Schools Coverage Period: 01/01/ /31/2017 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-582-6941. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-582-6941. Important Questions
Blue Choice Plan 2 Adobe Systems Incorporated
 Blue Choice Plan 2 Adobe Systems Incorporated Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: on or after 01/01/2014 Coverage for: Individual and Family Plan Type:
Blue Choice Plan 2 Adobe Systems Incorporated Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: on or after 01/01/2014 Coverage for: Individual and Family Plan Type:
Why This Matters: You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What This Plan Covers & What You Pay for Covered Services Coverage Period: on or after 01/01/2018 Blue Care Elect Saver with Coinsurance Teradyne, Inc. - HDHP with HSA
Summary of Benefits and Coverage: What This Plan Covers & What You Pay for Covered Services Coverage Period: on or after 01/01/2018 Blue Care Elect Saver with Coinsurance Teradyne, Inc. - HDHP with HSA
You don t have to meet deductibles for specific services.
 Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type:
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 Highmark Blue Shield: PPO Blue Coverage for: Individual/Family Plan Type: